By Mathew Keller, RN JD

Regulatory and Policy Nursing Specialist
Regulatory and Policy Nursing Specialist
Ask any Allina nurse. They all know why they are on strike. Health insurance, patient safety, workplace violence, and maintaining a voice in the workplace are all important aspects of this action. But what about Allina’s claims that the money it would save from cuts to nurses’ total compensation would be put to patient care?
As Allina puts it, the $10 million it proposes to take from nurses “means a whole lot to what service we’re able to provide,” according to Allina CEO Penny Wheeler. Unsurprisingly absent from that statement is why Allina needs this 10 million for patient care, why it needs to take it from its nurses, and why it can’t come from other sources.
As I mentioned in my previous blog, Allina Health’s Board of Directors is composed of investment bankers and non-healthcare company CEOs (even the CEO of Buffalo Wild Wings). Allina has made piles of money off of providing healthcare to the sickest amongst us.
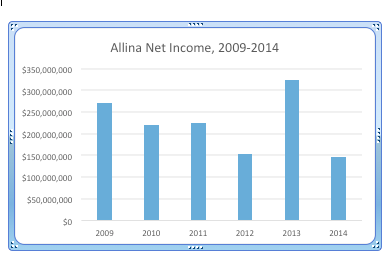
In fact, according to Allina Health’s annual financial disclosures as well as its consolidated financials (prepared by an “independent auditor” who sits on Allina’s Board), Allina Health has posted a net income after expenses of $1.3 billion over the past 6 years, including a net income of $271 million after expenses at the height of the recession in 2009 when most of the country was pinching pennies to get by. Allina hasn’t yet said why $10 million for patient care can’t come from those $1.3 billion dollars of net income.
Likewise, the top 25 paid executives at Allina health could take a cut to the $23.9 million dollars they made in 2014 in order to make up the $10 million. Or, the $10 million Allina suddenly needs for patient care could come from the $108 million it’s investing in a for-profit healthcare data analysis company, Health Catalyst, which happens to have Allina CEO Penny Wheeler on its Board of Directors.
The Health Catalyst transaction, notably, isn’t about improving patient care—it’s about cutting costs. As nurses can tell you, cost cutting in hospitals tends to come from one source: cutting nursing care. Because nursing care is rolled into the “bed fee,” patients pay the same whether they received the 10 hours of nursing care they needed or the four hours Allina decided it would give them. This creates a perverse financial incentive for hospitals to cut costs through cutting the main reason patients are in a hospital and not in an outpatient setting. The reason? Nursing care.
At the end of the day, that’s what this is all about: squeezing every penny Allina can out of its nurses, its other employees, and most importantly, out of its patients. You will pay the same at Allina Health regardless of the outcome of these negotiations and regardless of whether or not Allina fleeces $10 million out of its nurses. As a commentary from Rand Corp. put it, “unfortunately, nearly every actor in our health care delivery system — hospitals, physicians, other health care providers, insurance companies and the manufacturers of drugs and devices — is currently focused on maximizing revenue growth.”
Indeed, we’ve seen that no matter how much money Allina makes, it doesn’t return it to its customers. From fiscal years (FY) 2013-2014, when Allina made $470.3 million dollars after expenses, the amount of charitable care it provided actually decreased by 18 percent, and, rest assured, everything from the cost of a band-aid to the cost of a a splenectomy went up too. The argument that Allina and other Minnesota healthcare systems provide enough of a community benefit to even be considered non-profit anymore is so weak at this point that many commenters, including, notably, a medical director at Allina, believe the whole system deserves much greater scrutiny. Likewise, any claims from Allina that skimming $10 million from the total compensation of its nurses will improve patient care deserve greater scrutiny as well.

